Nutrition
An Intro To The Ketogenic Diet
Many people have heard about the ketogenic diet, but not many understand how it is or why someone would do it. This article breaks the ketogenic diet apart and interprets how it’s gotten some of its health claims.
May 14, 2018 · updated July 6, 2026

There are a ton of fad diets out there, and quite frankly, most of them are not what they’re advertised to be.
I’ve experimented with many of these diets on my own to test out what works for me, and identify which philosophies made the most sense to me from a biochemical standpoint.
Among all of the many diet philosophies out there; Atkins/Modified Atkins, Paleo, Vegan, Fruitarian, Alkaline, etc, the one that has stood out to me the most is the ketogenic diet.
Here I discuss the details of the diet, include some of the science surrounding it’s health claims, and a brief description of the biochemistry taking place in those following this diet philosophy.
As with anything, I encourage everyone to do their own research, and to remain skeptical. This is meant to serve as a starting point for those interested in delving deeper into the ketogenic diet.

What Is The Ketogenic Diet?
The ketogenic diet is designed to condition the body to use ketone bodies (from fat) as a primary source of fuel rather than glucose (from carbohydrates).
Achieving this involves eating roughly 70-75% of the total daily calorie intake in the form of fat, with protein making up around 20% and carbohydrates cut down to roughly 5-10% of daily calorie intake.
The goal of a ketogenic diet is to achieve a state of metabolic ketosis. The idea is that this essentially allows us to tap into a larger fuel tank (fat reserves) to supply more consistent energy levels throughout the day. It also allows for easy breakdown of fat stores for energy, making it easier to lose weight.
Cellular Energy Substrates
There are 2 groups of molecules the body uses as a substrate for energy production:
1. Sugars
Carbohydrates and complex sugars are absorbed from the digestive tract and converted to simple sugars (glucose and fructose). Insulin is then secreted into the bloodstream to shuttle sugars into the cells where they are converted into energy.
When blood glucose dips, stored glucose is broken down from glycogen in the muscles and liver.
2. Ketones
Ketones are released during a fasted state to provide energy to the cells in the absence of glucose. They are made from our dietary fats, as well as stored fats.
Unlike sugars, fats are not water soluble, and therefore cannot be released into the bloodstream in their raw forms. The liver converts stored fat to water soluble ketones such as acetoacetate and beta-hydroxybutyrate.
These ketones then travel throughout the body to be used as a substrate for energy production. They can enter the cells directly without the need for insulin.
Understanding Macronutrients:
There are 3 main macronutrients the body needs to survive, carbohydrates, proteins, and fats.
Carbohydrates
Carbohydrates can be thought of like rocket fuel. They’re converted into glucose in the digestive tract and absorbed into the bloodstream quickly. The energy from carbohydrates (especially simple carbohydrates) provide a lot of energy quickly, but tends to need refueling often to avoid crashing.
Proteins
Proteins can be thought of as the building blocks for the body. We break proteins down into their smallest pieces, amino acids, before absorbing them into the bloodstream. Our body then uses these proteins to build new cells, enzymes, hormones, and neurotransmitters. We can also convert proteins into glucose for energy, although this takes more time and energy investment to do, so the body only does this when glucose isn’t readily available.
Fats
Finally, we have fats, which are the basis of the ketogenic diet. Fats can be thought of as lumps of coal. They are a dense store of energy, which can be released more slowly over time. We rely on fats for energy during times of starvation. Instead of converting to glucose, however, fats are turned into a group of chemicals known as ketones.
Why Choose The Ketogenic Diet?
Blood glucose spikes after a meal
Many people choose the ketogenic diet for medical reasons (more on this below), most notably as a medically supervised therapy for drug-resistant epilepsy. Others explore it, with more mixed evidence behind it, for conditions such as type 2 diabetes, multiple sclerosis, or Alzheimer’s disease.
Others use it as part of a cognitive enhancement regimen, to improve athletic endurance, or to lose weight.
Perhaps the main reason people choose the ketogenic diet is to manage energy levels.
With carbohydrate-adapted metabolism, blood glucose tends to spike directly following a meal. The body responds to this by increasing insulin levels to shuttle these sugars into the cells. If we have more glucose than we do energy requirements, this excess glucose is converted to fat. Additionally, insulin inhibits the breakdown of fat, making it difficult to retrieve energy from fat stores. This results in spikes in energy after meals, followed by crashes soon after.
Keto-adapted metabolism, on the other hand, has a much slower breakdown and absorption into the blood stream, allowing the energy-dense fats to absorb slowly over time.
Additionally, keto-adapted metabolism involves low insulin levels, allowing the breakdown of fat to occur freely.
This allows fat to support periods of low dietary energy intake much more seamlessly than glucose. This is why one of the key features of keto-adaptation is low appetite, even after 10 to 16 hours of fasting.
Ketones appear to be a somewhat more efficient fuel than glucose, at least by some measures: gram for gram, the ketone body beta-hydroxybutyrate yields more ATP than glucose, and it produces more ATP per two-carbon unit metabolised. The advantage isn’t universal, however — by other measures, such as ATP generated per oxygen consumed, glucose and ketones are roughly comparable 12Reference 12Ketone body metabolism in the ischemic heart.
Research For Keto-Adaptation
Weight Loss
Traditional Diet
With traditional, high carb diets, fat burning only happens after all of our blood sugar and glycogen reserves have been used up. Exercise increases our bodies demand for energy, which it responds to by dumping more glucose into the blood from glycogen. When we exercise, we need to work for as long as 90 minutes with low intensity exercise, or 20 minutes of high intensity in order to deplete this glycogen. Only after this point will we begin burning fat for energy.
Ketogenic Diet
Despite what you might think, eating fat doesn’t make you gain fat. When we eat fat, we easily store excess energy in the form of fat, however, we also break it apart easily through an enzyme known as lipase. This enzyme is tasked with releasing fat into the bloodstream from the adipocyte storage cells.
When we are in ketosis, a careful control of our calorie intake makes it very easy to lose weight by converting stored fat to ketone bodies to use for energy, and makes our exercise routines more efficient because our bodies already begin breaking down fat for energy when demand increases.
Some Research
A meta-analysis of randomised controlled trials comparing very-low-carbohydrate ketogenic diets against low-fat diets found modestly greater long-term weight loss on the ketogenic side 1Reference 1Meta-analysisVery-low-carbohydrate ketogenic diet v. low-fat diet for long-term weight loss: a meta-analysis of randomised controlled trials. That said, a more recent umbrella review of 23 meta-analyses found the picture is more nuanced: ketogenic diets can also raise LDL and total cholesterol in some studies, and most trials only track outcomes for a few months to a year rather than years 2Reference 2Meta-analysisKetogenic diet and multiple health outcomes: an umbrella review of meta-analyses. Adherence is a recurring theme in the broader ketogenic-diet literature too — the diet’s strict macronutrient targets are hard to sustain long-term, and dropout tends to climb the longer the follow-up period. In other words, short-term results look promising, but the long-term picture is more mixed and depends heavily on whether people can actually stick with it.
Improved Focus & Concentration
The keto-adapted brain is thought to be more efficient than its carb-fueled counterpart. This idea partly comes from animal research showing that the ketone body D-β-hydroxybutyrate can increase BDNF, a protein that supports learning and memory 3Reference 3Exercise promotes the expression of brain-derived neurotrophic factor (BDNF) through the action of the ketone body β-hydroxybutyrate. eLife, 5, e15092.
+ Neuroprotection
The ketogenic diet has been studied for a variety of proposed neuroprotective mechanisms across conditions ranging from epilepsy, Alzheimer’s disease, and Parkinson’s disease, to multiple sclerosis, traumatic brain injury, and stroke. The strength of the evidence varies enormously between these — it’s well established for epilepsy, and much more preliminary and largely preclinical (animal or lab-based) for the rest.
Epilepsy is the one application with a genuinely strong evidence base and decades of clinical use, historically strongest in children with drug-resistant epilepsy. Multicentre studies have found meaningful seizure reduction in a substantial proportion of patients who don’t respond to medication 9Reference 9A multicenter study of the efficacy of the ketogenic diet. It is always used as a medically supervised therapy — under a neurologist and dietitian, with monitoring for side effects like constipation, kidney stones, and growth or lipid changes — not something to start unsupervised.
For the other conditions, the case is much earlier-stage. One line of reasoning is that ketones may offer the brain a more efficient fuel source when its ability to use glucose declines, which has been observed with ageing and in Alzheimer’s disease models 4Reference 4AnimalEarly decline in glucose transport and metabolism precedes shift to ketogenic system in female aging and Alzheimer’s mouse brain: implication for bioenergetic intervention. This has led to exploratory work on the diet’s potential relevance to Alzheimer’s disease itself 5Reference 5AnimalA ketogenic diet reduces amyloid beta 40 and 42 in a mouse model of Alzheimer’s disease, Parkinson’s disease 6Reference 6Treatment of Parkinson disease with diet-induced hyperketonemia: a feasibility study, multiple sclerosis 7Reference 7AnimalInflammation-mediated memory dysfunction and effects of a ketogenic diet in a murine model of multiple sclerosis, and traumatic or hypoxic brain injury 8Reference 8Neuroprotective and disease-modifying effects of the ketogenic diet — but this is mechanistic and early-stage evidence, mostly from animal models and small feasibility studies, not proof that the diet treats or prevents these conditions in people.
How Does Ketosis Work?
Metabolic ketosis involves an upregulation of processes related to fat breakdown (lipolysis) and mobilisation into the cells for energy. Fat contained in the fat storage cells (adipocytes) are converted from triglycerides to fatty acids, then into acetyl-coA (through beta-oxidation). These molecules are then converted into ketone bodies like Acetoacetate and 3-hydroxybutyrate in the liver.
Ketones are released into circulation from the liver because the liver is unable to use these ketones for itself. (It lacks the mitochondrial enzyme succinyl-CoA:3-ketoacid CoA transferase, which peripheral tissues need to reactivate acetoacetate back to acetoacetyl-CoA 10Reference 10F., Masood, W., Annamaraju, P., & Khan Suheb, M).
These ketones are then released into the blood to supply cells throughout the body with energy.
Although the body can convert protein to glucose through a process called gluconeogenesis, this process is undesired. This is because in order to supply the brain with the required 110-120g of glucose, roughly 160 to 200 g of protein (close to 1 kg of muscle tissue) needs to be broken down 11Reference 11Regulation of fuel utilization.
In order to prevent this from happening, the body is well adapted to begin using fats through ketosis when faced with low glucose availability. It does this in order to reduce the need to convert proteins to glucose instead, resulting in muscle wasting.
How Long Does It Take To Achieve Keto-Adaptation?
There are varying levels of ketosis. Early stages begin after about 2 days of hypoglycemia (low blood glucose). The body will become weak and energy deficient, gluconeogenesis increases to convert proteins to glucose, and lipolysis will begin to release acetyl-coa into the bloodstream towards the liver. The liver then converts this into ketones like acetoacetate.
After about a week, this process becomes increasingly efficient, and most people will reach a state of mild keto-adaptation by this point.
True keto-adaptation is considered to be between 1.5 and 3 mmol ketones per L of blood. This can take between 3 weeks, and 3 months, depending on the carbohydrate and protein intake. Genetic factors (such as PPARα and APOE variations) also play a role here, with some genetic variants allowing ketosis more readily than others.
Ideal Macronutrient Distribution
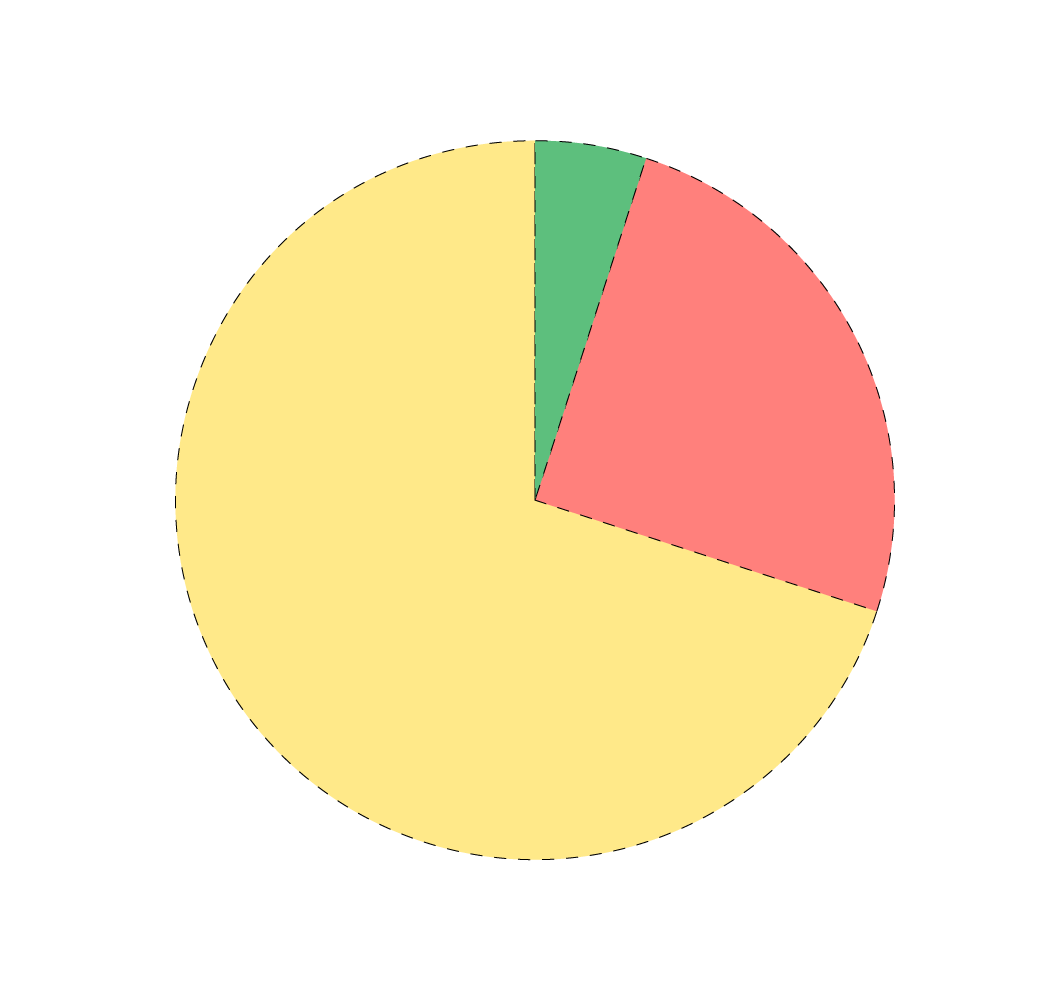
Energy intake distribution in %
Measuring macronutrients is the basis for the ketogenic diet. The standard target for most people is roughly 70-75% of total energy intake from fat, about 20% from protein, and 5-10% from carbohydrates.

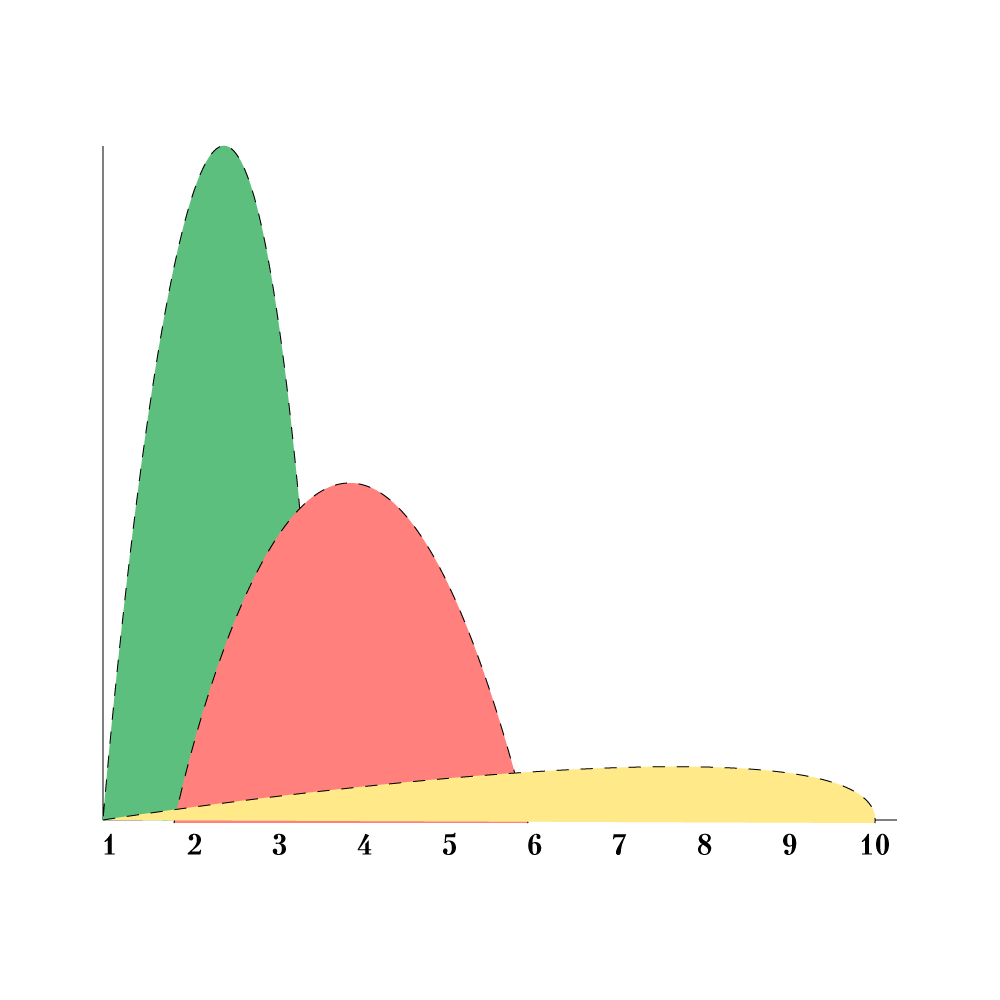
Energy in kJ per g
Fat Is High Energy
Fat contains roughly double the energy per gram than carbohydrates and proteins, it’s fairly easy to achieve this macronutrient distribution through the addition of vegetable and animal fats to meals.
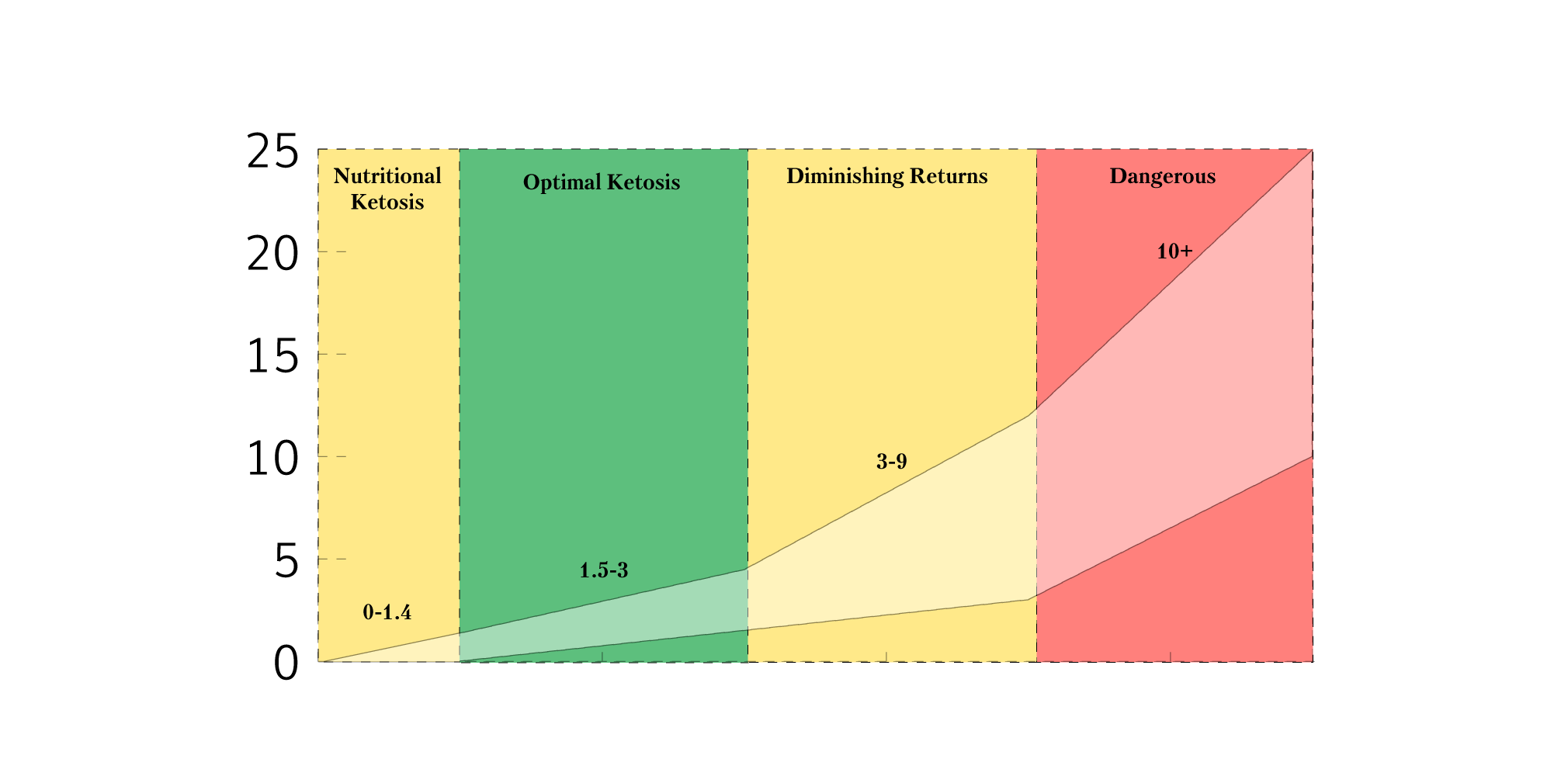
Measuring Ketosis
Ketosis is best measured by how you feel on the diet. Most people are able to tell when their body is in ketosis based on variations in their energy and hunger levels.
To measure ketosis with biometrics, testing ketone levels in the blood or urine can be done using urine dip sticks, or blood ketone sensors.
Optimal ketosis is considered to be within the range of 1.5 and 3 mmol/L of ketone bodies.
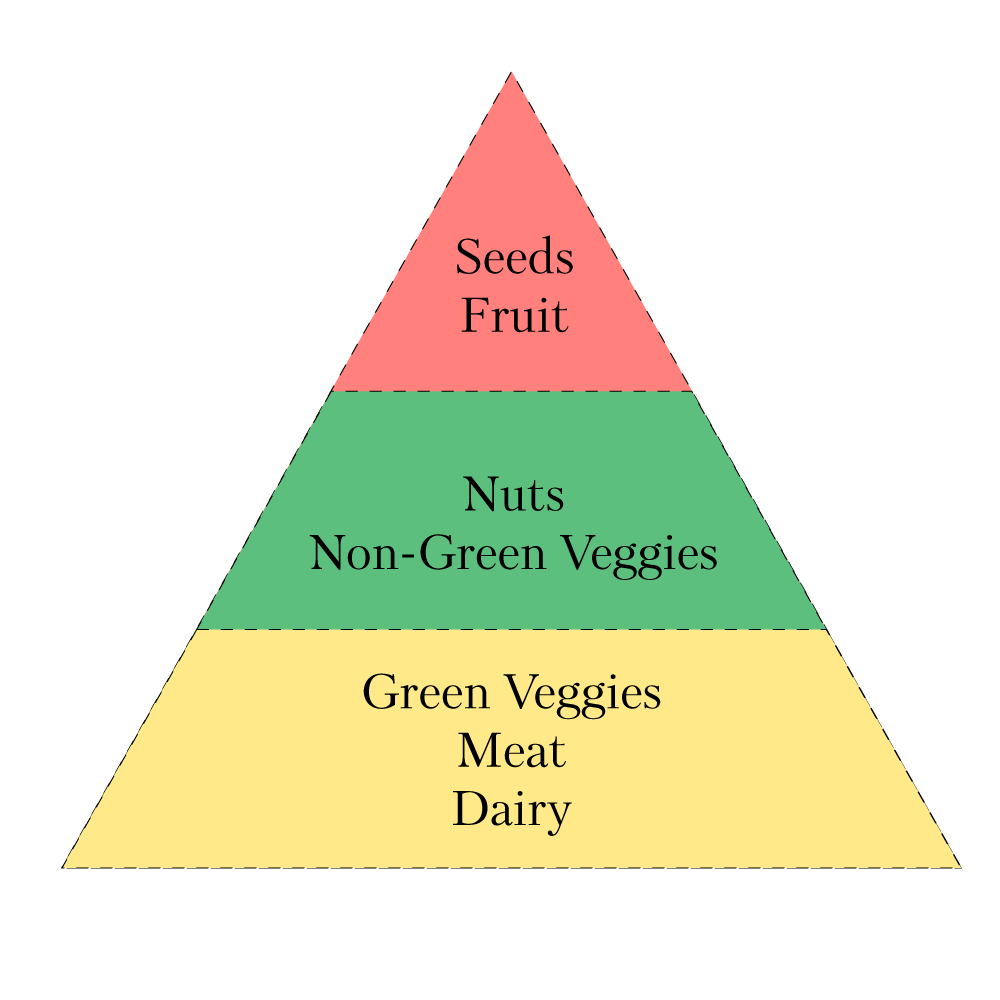
The keto food pyramid
References
- Bueno, N. B., de Melo, I. S. V., de Oliveira, S. L., & da Rocha Ataide, T. (2013). Very-low-carbohydrate ketogenic diet v. low-fat diet for long-term weight loss: a meta-analysis of randomised controlled trials. British Journal of Nutrition, 110(7), 1178–1187. Link
- Chen, S., Su, X., Feng, Y., Li, R., Liao, M., Fan, L., et al. (2023). Ketogenic diet and multiple health outcomes: an umbrella review of meta-analyses. Nutrients, 15(19), 4161. Link
- Sleiman, S. F., Henry, J., Al-Haddad, R., El Hayek, L., Abou Haidar, E., Stringer, T., et al. (2016). Exercise promotes the expression of brain-derived neurotrophic factor (BDNF) through the action of the ketone body β-hydroxybutyrate. eLife, 5, e15092. Link
- Ding, F., Yao, J., Rettberg, J. R., Chen, S., & Brinton, R. D. (2013). Early decline in glucose transport and metabolism precedes shift to ketogenic system in female aging and Alzheimer’s mouse brain: implication for bioenergetic intervention. PLoS ONE, 8(11), e79977. Link
- Van der Auwera, I., Wera, S., Van Leuven, F., & Henderson, S. T. (2005). A ketogenic diet reduces amyloid beta 40 and 42 in a mouse model of Alzheimer’s disease. Nutrition & Metabolism, 2(1), 28. Link
- VanItallie, T. B., Nonas, C., Di Rocco, A., Boyar, K., Hyams, K., & Heymsfield, S. B. (2005). Treatment of Parkinson disease with diet-induced hyperketonemia: a feasibility study. Neurology, 64(4), 728–730. Link
- Kim, D. Y., Hao, J., Liu, R., Turner, G., Shi, F. D., & Rho, J. M. (2012). Inflammation-mediated memory dysfunction and effects of a ketogenic diet in a murine model of multiple sclerosis. PLoS ONE, 7(5), e35476. Link
- Gasior, M., Rogawski, M. A., & Hartman, A. L. (2006). Neuroprotective and disease-modifying effects of the ketogenic diet. Behavioural Pharmacology, 17(5-6), 431–439. Link
- Vining, E. P. G., Freeman, J. M., Ballaban-Gil, K., Camfield, C. S., Camfield, P. R., Holmes, G. L., et al. (1998). A multicenter study of the efficacy of the ketogenic diet. Archives of Neurology, 55(11), 1433–1437. Link
- Daley, S. F., Masood, W., Annamaraju, P., & Khan Suheb, M. Z. Ketogenic diet. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing — covers hepatic ketogenesis and why the liver cannot itself use the ketone bodies it produces. Link
- Watford, M., & Goodridge, A. G. (2000). Regulation of fuel utilization. In Biochemical and Physiological Aspects of Human Nutrition. Philadelphia, PA: WB Saunders Company, 384–407.
- Kolwicz, S. C. Jr. (2021). Ketone body metabolism in the ischemic heart. Frontiers in Cardiovascular Medicine, 8, 789458. Link