
What Is Cannabis?
Cannabis is one of the most useful — and most versatile — plants in the herbal medicine cabinet. It’s best known for its psychoactive effects, but the same plant is a rich source of medicinal compounds that act on the endocannabinoid system, a signalling network the body uses to keep itself in balance. That’s what makes cannabis genuinely different from most herbs: it works through receptors that few other plants touch.
The plant produces more than a hundred cannabinoids, led by THC and CBD, alongside a fragrant layer of terpenes. Many of these compounds aren’t intoxicating at all — CBD in particular has become a mainstream supplement precisely because it delivers broad medicinal benefits without the “high.”
The one thing to understand up front is that cannabis is not a single drug. A high-CBD hemp oil, a high-THC flower, and a standardised THC:CBD extract behave like different medicines. Product, strain, and cannabinoid ratio make a real difference — so with cannabis, more than with almost any other herb, it matters which type you use for the job.
What Is Cannabis Used For?
Cannabis is reliably useful for a handful of things, and the effect depends heavily on the cannabinoid and terpene profile of what you’re using.
Cannabis is especially reliable for:
- Easing pain — particularly nerve pain and the aches of chronic conditions
- Calming muscle spasticity and cramping
- Settling nausea and stimulating appetite
- Lowering inflammation
- Improving sleep onset
- Reducing nervous excitability and, with CBD, anxiety
Cannabis works through a regulatory pathway rather than on one organ, which is why its effects can look bidirectional — it can both settle and stimulate depending on dose, chemotype and the person. THC is mildly stimulating at low doses and sedating at higher ones; THC stimulates appetite while THCV and CBD tend to suppress it. This is closer to how adaptogens like ginseng, ashwagandha or reishi produce their “it depends” results — though cannabis isn’t a true adaptogen (it doesn’t raise the body’s overall resistance to stress).
Because of that variability, strain and product choice is the whole game. Some cannabis extracts will ease anxiety; others, high in THC, can make it worse. An experienced herbalist or naturopath chooses the cannabinoid profile, terpene content and preparation to fit the person and the condition — rather than reaching for “cannabis” as a single thing.
Indications
- Chronic and neuropathic pain
- Multiple sclerosis (muscle spasticity)
- Chemotherapy-associated nausea
- Drug-resistant epilepsy (purified CBD)
- Anxiety (CBD)
- Insomnia
- Inflammatory bowel disease (symptom relief)
- Poor appetite / cachexia
- Menstrual cramping
- Arthritis and gout
- Substance-use recovery (CBD for cannabis use disorder)
Traditional Uses
Cannabis has one of the longest medicinal track records of any plant. It appears in the Chinese materia medica attributed to Shen Nong some two thousand years ago, and in Indian Ayurvedic practice — where bhang, a milk-and-cannabis preparation, was used for pain, sleep, digestion and as a nervous-system tonic. Across the Middle East, Africa and later Europe, the resin and flowers were used for much the same cluster of complaints: pain, cramping, poor sleep, and low appetite.
Cannabis was also a fixture of Western medicine. From the mid-1800s, after William O’Shaughnessy introduced it to British practice from India, cannabis tinctures were standard pharmacy items for pain, spasm, migraine and insomnia — right up until prohibition pushed the plant out of the pharmacopoeias in the early twentieth century.

A brief history
The plant’s usefulness and its fibre made it one of humanity’s oldest crops — hemp was grown for rope, cloth, paper and seed-oil for millennia before its medicine was formalised. Medicinal use is documented in ancient China and India, spread through the Islamic world, and entered European and American medicine in the 1800s as a mainstream remedy for pain, spasm and sleep.
Twentieth-century prohibition halted both use and research for decades. The modern revival began with the discovery of the endocannabinoid system in the late 1980s and 1990s — the receptors and signalling molecules that cannabis compounds act on — which finally gave a mechanism to centuries of anecdote. The last two decades have brought the first cannabis-derived licensed medicines (purified CBD for epilepsy, a THC:CBD spray for MS) and a wave of clinical research, even as whole-plant use has moved back into the legal mainstream in much of the world.
Phytochemistry
Cannabis is chemically dense: more than 550 compounds have been identified in the plant, including over 100 cannabinoids — the class of molecules, largely unique to cannabis, that resemble the body’s own endocannabinoids (anandamide and 2-AG) closely enough to act on the same receptors. The great majority of the plant’s effects come down to how these cannabinoids engage the CB1 receptors (concentrated in the nervous system) and CB2 receptors (concentrated in immune tissue), plus a set of non-cannabinoid targets.
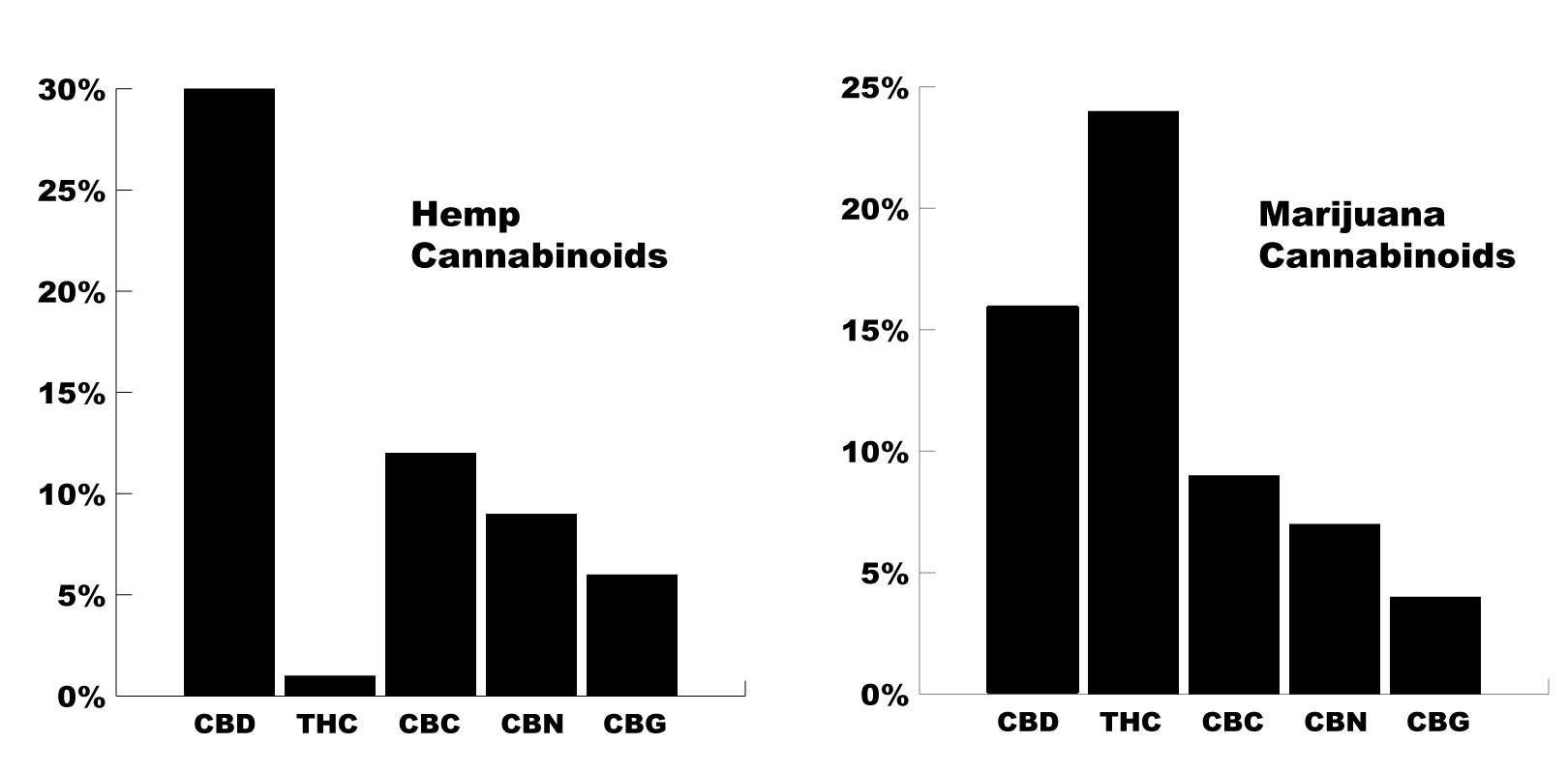
Just six cannabinoids — THC, CBD, CBG, CBC, CBN and THCV — account for the overwhelming bulk of the cannabinoid fraction. Which of them dominates is set almost entirely by chemotype: fibre-type hemp is CBD-dominant with THC below the ~0.3% legal threshold, while marijuana chemotypes are THC-dominant, and selective breeding can produce almost any ratio in between.
Layered on top are the aromatic terpenes — chiefly myrcene, limonene, beta-caryophyllene and pinene — which give each cultivar its scent and are thought to shade its effects.
Notable cannabinoids — what each one does
Cannabis’s effects are the sum of many cannabinoids, not just THC. The binding activity varies widely from one to the next — some act on CB1, some on CB2, some on neither — which is why the profile matters so much. The main players, in rough order of abundance:
- THC (tetrahydrocannabinol) — the principal psychoactive cannabinoid and a direct agonist at both CB1 and CB2 receptors. Beyond the “high,” it drives appetite stimulation, anti-nausea and analgesic effects, and is mildly stimulating at low doses, sedating at higher ones. Delta-9-THC is the abundant form; the closely related delta-8-THC occurs in small amounts.
- CBD (cannabidiol) — usually the other dominant cannabinoid, and non-intoxicating. It works largely around the CB1 receptor rather than on it: a 5-HT1A (serotonin) agonist, TRPV1 vanilloid-receptor agonist, FAAH inhibitor (raising the body’s own anandamide) and PPARγ activator. This broad, gentle profile underlies its anti-inflammatory, anxiolytic, anticonvulsant and mildly sedative reputation.
- CBG (cannabigerol) — the non-psychoactive precursor from which many other cannabinoids are made, so early-harvested plants are richer in it. An α2-adrenoceptor agonist and CB1/CB2 agonist with anti-inflammatory activity; often described as calming and less likely to provoke anxiety than THC.
- CBC (cannabichromene) — the third most abundant cannabinoid, non-psychoactive, acting mainly on the TRP vanilloid channels (TRPV3/TRPV4). Preclinical work points to anti-inflammatory and mild antidepressant effects, though human evidence is still thin.
- CBN (cannabinol) — formed as THC ages and breaks down, so older or heat-exposed material is higher in it. Mildly psychoactive at most, a weak CB1 agonist, and widely reputed as the most sedating of the group — a common choice for sleep, though controlled data are limited.
- THCV (tetrahydrocannabivarin) — chemically a near-twin of THC (two carbons shorter) with much weaker psychoactivity, roughly a quarter of THC’s potency. Notably an appetite suppressant, the opposite of THC.
The remaining cannabinoids — CBDV, CBGV, CBCV, CBL, CBE, CBGM, CBT and CBV — occur in small amounts and are mostly mapped chemically rather than studied for effect.
A quick word on synthetic cannabinoids (the street drug “spice” and similar): these lab-made compounds bind the same receptors but far more strongly and unpredictably, and they lack cannabis’s natural buffering. They cause serious harm — agitation, psychosis, seizures, heart attacks and deaths — and should be avoided entirely. They have nothing in common with the plant beyond the receptor they hit.

Cannabis Terpenes
The terpenes are the volatile, aromatic oils that give cannabis its smell — and they aren’t just for flavour. Cannabis shares many of them with pine, citrus, lavender and hops, and they carry mild medicinal activity of their own: anti-inflammatory, calming, antimicrobial. Beta-caryophyllene is a standout, being the one dietary terpene that acts directly on the CB2 cannabinoid receptor. The idea that terpenes and cannabinoids work together — the so-called “entourage effect” — is plausible and popular, though still mostly untested in humans.
Constituent Summary
Cannabinoid figures are % of dried flower and are strongly chemotype-dependent (hemp is CBD-dominant, marijuana THC-dominant). Terpene figures are % of dried flower within a typical ~1–4% total terpene fraction. Most minor cannabinoids and terpenes have no consistent published figure and are marked “No Data.”
Cannabinoids
Cannabinoid14 compounds2 with data
Terpenoids
Monoterpene17 compounds3 with data
Sesquiterpene7 compoundsno data
Diterpene1 compoundno data
Pharmacology & Research
Cannabis is one of the most heavily studied medicinal plants in the modern literature, and — unusually for a botanical — it reaches the top evidence tier for a handful of uses: purified cannabidiol (Epidiolex) and the whole-plant THC:CBD spray nabiximols (Sativex) are licensed medicines backed by pivotal randomised controlled trials and Cochrane-level meta-analysis 1,2,3,4,6,8Reference 1Meta-analysisCannabinoids for Medical Use: A Systematic Review and Meta-analysisView study →Reference 2RCTTrial of Cannabidiol for Drug-Resistant Seizures in the Dravet Syndrome — randomised controlled trialView study →Reference 3RCTEffect of Cannabidiol on Drop Seizures in the Lennox-Gastaut Syndrome — randomised controlled trialView study →Reference 4RCTCannabidiol in patients with seizures associated with Lennox-Gastaut syndrome (GWPCARE4) — randomised controlled trialView study →Reference 6Meta-analysisMeta-analysis of the efficacy and safety of Sativex (nabiximols) on spasticity in people with multiple sclerosisView study →Reference 8Systematic reviewCannabis and cannabinoids for symptomatic treatment for people with multiple sclerosis — Cochrane systematic reviewView study →. Beyond those, the evidence for the common consumer uses (pain, sleep, anxiety) is real but more modest 1,9,11Reference 1Meta-analysisCannabinoids for Medical Use: A Systematic Review and Meta-analysisView study →Reference 9Systematic reviewCannabis-based medicines for chronic neuropathic pain in adults — Cochrane systematic reviewView study →Reference 11RCTCannabidiol reduces the anxiety induced by simulated public speaking in treatment-naive social phobia patients — randomised controlled trialView study →. One thread runs through all of it: “cannabis” is not one drug — a high-CBD hemp oil, a high-THC flower, an isolated cannabinoid and a standardised extract behave differently, so the preparation matters as much as the dose.
- Best-supported: purified cannabidiol reduces seizures in Dravet and Lennox-Gastaut epilepsy (FDA/EMA-approved) 2,3,4Reference 2RCTTrial of Cannabidiol for Drug-Resistant Seizures in the Dravet Syndrome — randomised controlled trialView study →Reference 3RCTEffect of Cannabidiol on Drop Seizures in the Lennox-Gastaut Syndrome — randomised controlled trialView study →Reference 4RCTCannabidiol in patients with seizures associated with Lennox-Gastaut syndrome (GWPCARE4) — randomised controlled trialView study →; nabiximols eases multiple-sclerosis spasticity 6,8Reference 6Meta-analysisMeta-analysis of the efficacy and safety of Sativex (nabiximols) on spasticity in people with multiple sclerosisView study →Reference 8Systematic reviewCannabis and cannabinoids for symptomatic treatment for people with multiple sclerosis — Cochrane systematic reviewView study →; cannabinoids modestly reduce chronic neuropathic pain and chemotherapy nausea 9,10Reference 9Systematic reviewCannabis-based medicines for chronic neuropathic pain in adults — Cochrane systematic reviewView study →Reference 10Systematic reviewCannabinoids for nausea and vomiting in adults with cancer receiving chemotherapy — Cochrane systematic reviewView study →.
- Emerging, worth watching: cannabidiol for cannabis use disorder 12Reference 12RCTCannabidiol for the treatment of cannabis use disorder: a phase 2a, double-blind, placebo-controlled, randomised trialView study → and for symptom relief in Crohn’s disease 13,14Reference 13RCTOral CBD-rich Cannabis Induces Clinical but Not Endoscopic Response in Patients with Crohn’s Disease — randomised controlled trialView study →Reference 14Meta-analysisCannabis use in Crohn’s disease: a systematic review and meta-analysis of randomised controlled trialsView study →; CBD-based calm in acute-stress settings 11Reference 11RCTCannabidiol reduces the anxiety induced by simulated public speaking in treatment-naive social phobia patients — randomised controlled trialView study →.
- Thinner so far: standalone insomnia 17,18Reference 17RCTEffects of a cannabidiol/terpene formulation on sleep in individuals with insomnia: a double-blind, placebo-controlled randomised trialView study →Reference 18Meta-analysisEffectiveness of cannabinoids on subjective sleep quality in people with and without insomnia — systematic review and meta-analysisView study →; glaucoma (THC lowers eye pressure, but only for 3–4 hours) 20Reference 20RCTSingle oral administration of dronabinol increases ocular blood flow in patients with glaucoma — randomised controlled trialView study →; anticancer activity (striking in the lab, unproven in people) 21,22Reference 21Clinical trialA pilot clinical study of delta-9-tetrahydrocannabinol in patients with recurrent glioblastoma multiforme — clinical trialView study →Reference 22ReviewMechanisms of Cell Death Induced by Cannabidiol Against Tumor Cells: A Review of Preclinical StudiesView study →.
- Practical note: the cannabinoid ratio and preparation drive the effect, so match the product to the goal — high-CBD for calm and inflammation, THC-containing for pain, nausea and appetite.
0. Evidence by indication
Support is an experimental score I’m building — a composite weighted by study type (human > animal > in vitro > review) and study volume. It’s a beta: a fast way to rank strength of evidence at a glance, not a validated metric, and I’ll keep honing the formula over time. Each indication name links down to its write-up.
| Indication | Support | Rests on |
|---|---|---|
| Drug-resistant epilepsy | █████████░ 88% | Pivotal placebo-controlled RCTs of purified CBD in Dravet & Lennox-Gastaut; FDA/EMA-approved (Epidiolex). Syndrome-specific. |
| MS spasticity | ████████░░ 78% | Multiple RCTs & meta-analyses of nabiximols (Sativex); approved in many countries. Effect modest, partly subjective. |
| Chemotherapy nausea & vomiting | ███████░░░ 70% | Licensed synthetic THC (dronabinol/nabilone); Cochrane-reviewed, mostly older trials. |
| Chronic & neuropathic pain | ███████░░░ 66% | Many RCTs & Cochrane reviews; consistent but small effect; cancer pain largely null. |
| Anxiety | █████░░░░░ 48% | Small CBD RCTs in acute-stress/social-anxiety models; whole-plant THC can worsen it. |
| Cannabis use disorder | █████░░░░░ 45% | One well-conducted phase 2a CBD trial (positive); awaiting replication. |
| Inflammatory bowel disease | ████░░░░░░ 44% | RCTs show symptom & quality-of-life gains but no mucosal healing. |
| Appetite & cancer cachexia | ████░░░░░░ 42% | Older dronabinol data in HIV wasting; cancer-cachexia trials largely null. |
| Sleep / insomnia | ████░░░░░░ 41% | Small RCTs and a 2025 meta-analysis; modest, often secondary to pain relief. |
| Tourette syndrome & tics | ████░░░░░░ 38% | THC:CBD signals in small trials; the largest RCT missed its primary endpoint. |
| Glaucoma | ███░░░░░░░ 30% | THC lowers intraocular pressure but only ~3–4 h; not a practical therapy. |
| Anticancer | ███░░░░░░░ 28% | Strong in-vitro/animal mechanism; the one human pilot showed no survival benefit. |
1. Drug-resistant epilepsy
This is cannabis’s strongest evidence, and it rests on a single purified molecule. Two placebo-controlled RCTs of pharmaceutical cannabidiol (Epidiolex, added to existing anti-seizure drugs) cut convulsive seizures in Dravet syndrome by roughly 39% versus 13% on placebo 2Reference 2RCTTrial of Cannabidiol for Drug-Resistant Seizures in the Dravet Syndrome — randomised controlled trialView study →, and drop-seizures in Lennox-Gastaut syndrome fell about 42–44% versus ~17–22% at 10–20 mg/kg/day 3,4Reference 3RCTEffect of Cannabidiol on Drop Seizures in the Lennox-Gastaut Syndrome — randomised controlled trialView study →Reference 4RCTCannabidiol in patients with seizures associated with Lennox-Gastaut syndrome (GWPCARE4) — randomised controlled trialView study →. A 2025 meta-analysis confirms a consistent, dose-related reduction in seizure frequency 5Reference 5Meta-analysisCannabis derivatives and their synthetic analogs for treatment-resistant epilepsy — systematic review and meta-analysisView study →. Worth knowing: this benefit is established for high-dose purified CBD in these specific syndromes — not for consumer CBD oils or smoked cannabis.
2. MS spasticity
Nabiximols — a standardised 1:1 THC:CBD oromucosal spray — is licensed in many countries for multiple-sclerosis spasticity that resists first-line drugs. A meta-analysis of the pivotal RCTs found a modest but reproducible reduction in patient-rated spasticity, with a subset of “responders” gaining meaningful relief 6Reference 6Meta-analysisMeta-analysis of the efficacy and safety of Sativex (nabiximols) on spasticity in people with multiple sclerosisView study →, and a 2023 meta-analysis supports it as add-on therapy 7Reference 7Meta-analysisNabiximols is Efficient as Add-On Treatment for Patients with Multiple Sclerosis Spasticity Refractory to Standard Treatment — systematic review and meta-analysisView study →. The 2022 Cochrane review rates the evidence low-to-moderate certainty with a small average effect 8Reference 8Systematic reviewCannabis and cannabinoids for symptomatic treatment for people with multiple sclerosis — Cochrane systematic reviewView study → — patient-reported spasticity improves more than examiner-rated measures.
3. Chemotherapy nausea & vomiting
Synthetic THC analogues — dronabinol and nabilone — have been licensed antiemetics since the 1980s, making this one of cannabis’s oldest evidence-based uses. A Cochrane review found cannabinoids more effective than placebo and broadly comparable to older antiemetics for chemotherapy-induced nausea, and often the treatment patients preferred 10Reference 10Systematic reviewCannabinoids for nausea and vomiting in adults with cancer receiving chemotherapy — Cochrane systematic reviewView study →. Modern 5-HT3 antagonists have largely taken over as first-line, so cannabinoids now sit as an option for nausea that resists standard drugs — a role the 2024 ASCO guideline endorses 26Reference 26Cannabis and Cannabinoids in Adults With Cancer: ASCO Guideline — practice guidelineView study →.
4. Chronic & neuropathic pain
Pain is the most common reason people reach for medicinal cannabis. Across many RCTs and a 2026 Cochrane review, cannabis-based medicines produce a small reduction in chronic neuropathic pain, with sedation and dizziness as common trade-offs 9Reference 9Systematic reviewCannabis-based medicines for chronic neuropathic pain in adults — Cochrane systematic reviewView study →. The umbrella JAMA meta-analysis rated the overall pain evidence moderate-quality 1Reference 1Meta-analysisCannabinoids for Medical Use: A Systematic Review and Meta-analysisView study →. One clean exception is worth flagging: in cancer pain specifically, a 2023 Cochrane review found little or no benefit over placebo 23Reference 23Systematic reviewCannabis-based medicines and medical cannabis for adults with cancer pain — Cochrane systematic reviewView study →. Cannabis is a reasonable option for stubborn nerve pain, but it’s a modest analgesic, not a strong one.
5. Anxiety
The calming story belongs to cannabidiol, not the whole plant — high-THC cannabis can provoke anxiety and paranoia. In a double-blind RCT, a single 600 mg oral CBD dose reduced anxiety during a simulated public-speaking test in people with social anxiety 11Reference 11RCTCannabidiol reduces the anxiety induced by simulated public speaking in treatment-naive social phobia patients — randomised controlled trialView study →, and several smaller acute-dosing studies point the same way. The catch for consumers: these effects showed up at 300–600 mg CBD, far above the 10–50 mg in most retail products, and there’s no large trial yet of sustained CBD dosing for a diagnosed anxiety disorder.
6. Cannabis use disorder
Counterintuitively, cannabidiol shows promise for helping people cut down on cannabis itself. In a phase 2a double-blind RCT, 400 mg and 800 mg daily CBD beat placebo on measures of cannabis use in people with moderate-to-severe cannabis use disorder 12Reference 12RCTCannabidiol for the treatment of cannabis use disorder: a phase 2a, double-blind, placebo-controlled, randomised trialView study →. It’s a single, well-designed trial — a credible signal that now needs replication in a larger group.
7. Inflammatory bowel disease
People with Crohn’s disease and ulcerative colitis widely use cannabis for relief, and the trials capture a specific pattern: symptoms and quality of life improve, but the underlying inflammation doesn’t. An RCT of oral CBD-rich cannabis in Crohn’s produced clinical improvement without endoscopic (mucosal) healing 13Reference 13RCTOral CBD-rich Cannabis Induces Clinical but Not Endoscopic Response in Patients with Crohn’s Disease — randomised controlled trialView study →, and a 2025 meta-analysis reaches the same split conclusion 14Reference 14Meta-analysisCannabis use in Crohn’s disease: a systematic review and meta-analysis of randomised controlled trialsView study →. That makes cannabis a useful symptomatic adjunct rather than a replacement for disease-modifying IBD treatment.
8. Appetite & cancer cachexia
The appetite-stimulating “munchies” effect is real — THC drives appetite through CB1 receptors — and older dronabinol trials supported it in HIV-associated wasting. In cancer cachexia, though, the controlled trials are largely null: cannabinoids didn’t outperform placebo or megestrol for appetite or weight 15,16Reference 15Meta-analysisSystematic review and meta-analysis of cannabinoids in palliative medicineView study →Reference 16Meta-analysisEfficacy of medicinal cannabis for appetite-related symptoms in people with cancer — systematic review and meta-analysisView study →. So the appetite effect is genuine pharmacologically but unreliable in the setting where it’s most needed.
9. Sleep / insomnia
Many people use cannabis for sleep, and a 2025 meta-analysis found cannabinoids modestly improve subjective sleep quality — with the strongest signal where insomnia is secondary to pain or another chronic condition rather than primary 18Reference 18Meta-analysisEffectiveness of cannabinoids on subjective sleep quality in people with and without insomnia — systematic review and meta-analysisView study →. A small phase 2 RCT of a CBD/terpene formula also improved insomnia symptoms 17Reference 17RCTEffects of a cannabidiol/terpene formulation on sleep in individuals with insomnia: a double-blind, placebo-controlled randomised trialView study →. Much of the benefit seems to flow from easing pain or anxiety, and regular THC use builds tolerance to the sedative effect.
10. Tourette syndrome & tics
Case series and small studies have long suggested THC reduces tics, and small THC:CBD studies report improvement. But CANNA-TICS, the largest RCT of nabiximols in chronic tic disorders, did not meet its primary endpoint, with only secondary analyses hinting at benefit in a subgroup 19Reference 19RCTCANNA-TICS: Efficacy and safety of oral treatment with nabiximols in adults with chronic tic disorders — randomised controlled trialView study →. A promising signal that the best-powered trial so far couldn’t confirm.
11. Glaucoma
A textbook case of a real effect that isn’t practical. THC does lower intraocular pressure — but only for about 3–4 hours, which would mean near-constant dosing (and near-constant intoxication), so ophthalmology bodies don’t recommend it. Newer work is exploring pressure-independent routes: a 2026 RCT found a single oral dronabinol dose increased ocular blood flow in glaucoma patients 20Reference 20RCTSingle oral administration of dronabinol increases ocular blood flow in patients with glaucoma — randomised controlled trialView study →, a mechanism of interest rather than an established therapy.
12. Anticancer
Cannabis’s antitumour reputation rests almost entirely on laboratory work: in cell and animal studies, CBD and THC can trigger cancer-cell death across several tumour types 22Reference 22ReviewMechanisms of Cell Death Induced by Cannabidiol Against Tumor Cells: A Review of Preclinical StudiesView study →. The one human test — a 2006 pilot infusing THC into recurrent glioblastoma in nine patients — established safety but showed no survival benefit 21Reference 21Clinical trialA pilot clinical study of delta-9-tetrahydrocannabinol in patients with recurrent glioblastoma multiforme — clinical trialView study →. The gap between striking petri-dish results and the absence of human efficacy is the whole story here; cannabis is not a cancer treatment.
Mechanisms
| Mechanism | Drives | Key compounds |
|---|---|---|
| CB1 receptor agonism (CNS) | psychoactivity, analgesia, appetite, antiemetic | THC |
| CB2 receptor agonism (immune tissue) | anti-inflammatory, immunomodulation | THC, CBG |
| CB1-independent: 5-HT1A agonism, TRPV1/2 agonism, FAAH & adenosine-reuptake inhibition | anxiolytic, anti-inflammatory, neuroprotective | CBD |
| GPR55 antagonism, voltage-gated & T-type Ca²⁺ channel modulation | anticonvulsant | CBD |
| PPARγ nuclear-receptor activation | anti-inflammatory, neuroprotective, antitumour | THC, CBD |
| TRPA1 agonism / TRPM8 antagonism | analgesic, anti-inflammatory | CBG, CBC |
Clinical trials
Cannabis has one of the largest clinical-trial footprints of any plant medicine — roughly 1,290 completed and 520 recruiting or planned studies registered on ClinicalTrials.gov across all cannabinoids, alongside two syndrome-specific FDA approvals (Epidiolex for epilepsy) and multi-country licensing of nabiximols. The caveat is that most completed trials are small and vary widely in preparation.
| Completed | Planned | Terminated | Preclinical |
|---|---|---|---|
| ~1,290 | ~520 | ~235 | thousands |
Last checked: July 2026.
Dosage
There’s no single cannabis dose — it depends entirely on the preparation and the cannabinoid you’re after. As a rough anchor, everyday CBD supplement use tends to land in the range of 70–700 mg of CBD per day, but the clinically studied doses run higher and vary by goal (see the table). For THC-containing products, the golden rule is start low and go slow: a small amount, wait, and titrate up — the psychoactive and side effects climb quickly once you pass your comfortable dose.
Because whole-plant potency swings enormously with chemotype, always follow the product’s own labelling over any generic figure, and give inhaled or oral doses time to take effect before redosing (oral onset can take 1–2 hours).
The doses below are what the studies actually used — largely purified isolates or standardised pharmaceutical extracts, not whole flower — so they’re a reference, not a recommendation.
| Indication | Preparation | Dose | Source |
|---|---|---|---|
| Drug-resistant epilepsy | Purified CBD oral solution (Epidiolex) | 10–20 mg/kg/day | 2,3,4Reference 2RCTTrial of Cannabidiol for Drug-Resistant Seizures in the Dravet Syndrome — randomised controlled trialView study →Reference 3RCTEffect of Cannabidiol on Drop Seizures in the Lennox-Gastaut Syndrome — randomised controlled trialView study →Reference 4RCTCannabidiol in patients with seizures associated with Lennox-Gastaut syndrome (GWPCARE4) — randomised controlled trialView study → |
| MS spasticity | Nabiximols spray (2.7 mg THC + 2.5 mg CBD/spray) | up to ~12 sprays/day, self-titrated | 6,8Reference 6Meta-analysisMeta-analysis of the efficacy and safety of Sativex (nabiximols) on spasticity in people with multiple sclerosisView study →Reference 8Systematic reviewCannabis and cannabinoids for symptomatic treatment for people with multiple sclerosis — Cochrane systematic reviewView study → |
| Chemotherapy nausea | Dronabinol (synthetic THC) | ~5 mg/m² per dose | 10Reference 10Systematic reviewCannabinoids for nausea and vomiting in adults with cancer receiving chemotherapy — Cochrane systematic reviewView study → |
| Anxiety (acute) | Purified CBD, single oral dose | 300–600 mg | 11Reference 11RCTCannabidiol reduces the anxiety induced by simulated public speaking in treatment-naive social phobia patients — randomised controlled trialView study → |
| Cannabis use disorder | Purified CBD, oral, daily | 400–800 mg/day | 12Reference 12RCTCannabidiol for the treatment of cannabis use disorder: a phase 2a, double-blind, placebo-controlled, randomised trialView study → |
| Crohn’s (symptomatic) | CBD-rich cannabis oil | ~320 mg CBD/day | 13Reference 13RCTOral CBD-rich Cannabis Induces Clinical but Not Endoscopic Response in Patients with Crohn’s Disease — randomised controlled trialView study → |
These effective doses come from purified isolates or standardised extracts, so they don’t back-convert to a weight of dried flower — whole-plant cannabinoid content and absorption differ far too much by chemotype to imply an equivalence.
Traditional Dosage
| System | Preparation | Dose |
|---|---|---|
| Western herbal (CBD supplement basis) | CBD oil / extract | ~70–700 mg CBD/day |
| Whole flower (inhaled / vaporised) | smoked or vaporised flower | dose to effect; highly chemotype-dependent |
| Traditional oral (e.g. bhang) | milk/fat infusion of flower & leaf | prepared to strength; effect delayed and long-lasting |
Safety
Used sensibly, cannabis has a wide margin — there’s no known lethal dose of the whole plant, and most side effects are dose-related and pass on their own. The things worth actually paying attention to are these:
It’s psychoactive, so don’t drive on it. THC impairs coordination, reaction time and judgement, and impaired driving is one of the best-established acute harms. High doses can also tip into anxiety, panic or transient paranoia — more likely with high-THC, low-CBD material.
Regular use can build tolerance and mild dependence. Roughly one in ten users develop some degree of cannabis use disorder, more with early-onset or daily heavy use. Taking periodic breaks keeps tolerance in check.
Mind the drug interactions. CBD inhibits several liver enzymes (CYP3A4, CYP2C9, CYP2C19, CYP2D6, CYP1A2), so it can raise blood levels of other medications — the interaction with the epilepsy drug clobazam is the best-documented — and high-dose CBD can nudge up liver enzymes. Combining cannabis with alcohol, benzodiazepines or opioids adds to their sedation. If you take prescription medicine, check with your doctor or pharmacist first.
A few groups should be cautious. Anyone with a personal or family history of psychosis or schizophrenia should avoid high-potency cannabis, as heavier use is consistently linked to a higher risk of psychotic illness 24Reference 24Meta-analysisMeta-analysis of the Association Between the Level of Cannabis Use and Risk of PsychosisView study →. People with cardiovascular disease should be careful too, since THC raises heart rate and can affect blood pressure. And smoking anything irritates the lungs — vaporising or oral use avoids the bronchitis and cough that come with smoke.
Legality varies widely and changes often — from fully legal to strictly prohibited depending on country and state — so check the rules where you live before buying or carrying cannabis.
Potential Side-Effects
- Dry mouth and dry/red eyes
- Dizziness or lightheadedness
- Increased appetite
- Fatigue or drowsiness
- Anxiety or paranoia (usually high-THC)
- Rapid heartbeat / palpitations
- Short-term memory and coordination effects
- Nausea (occasionally, especially high doses)
- Cough or bronchitis (smoking only)
Pregnancy & lactation
Avoid. Prenatal cannabis exposure is associated with adverse neonatal outcomes including lower birth weight and a greater likelihood of neonatal intensive-care admission 25Reference 25Meta-analysisFetal Cannabis Exposure and Neonatal Outcomes: A Systematic Review and Meta-AnalysisView study →, and THC crosses the placenta and passes into breast milk. Cannabis isn’t recommended during pregnancy or breastfeeding.
References
- Whiting, P. F., Wolff, R. F., Deshpande, S., et al. (2015). Cannabinoids for Medical Use: A Systematic Review and Meta-analysis. JAMA. https://pubmed.ncbi.nlm.nih.gov/26103030/
- Devinsky, O., Cross, J. H., Laux, L., et al. (2017). Trial of Cannabidiol for Drug-Resistant Seizures in the Dravet Syndrome — randomised controlled trial. New England Journal of Medicine. https://pubmed.ncbi.nlm.nih.gov/28538134/
- Devinsky, O., Patel, A. D., Cross, J. H., et al. (2018). Effect of Cannabidiol on Drop Seizures in the Lennox-Gastaut Syndrome — randomised controlled trial. New England Journal of Medicine. https://pubmed.ncbi.nlm.nih.gov/29768152/
- Thiele, E. A., Marsh, E. D., French, J. A., et al. (2018). Cannabidiol in patients with seizures associated with Lennox-Gastaut syndrome (GWPCARE4) — randomised controlled trial. The Lancet. https://pubmed.ncbi.nlm.nih.gov/29395273/
- (2025). Cannabis derivatives and their synthetic analogs for treatment-resistant epilepsy — systematic review and meta-analysis. Epilepsy Research. https://pubmed.ncbi.nlm.nih.gov/40267856/
- Wade, D. T., Collin, C., Stott, C., & Duncombe, P. (2010). Meta-analysis of the efficacy and safety of Sativex (nabiximols) on spasticity in people with multiple sclerosis. Multiple Sclerosis Journal. https://pubmed.ncbi.nlm.nih.gov/20558502/
- (2023). Nabiximols is Efficient as Add-On Treatment for Patients with Multiple Sclerosis Spasticity Refractory to Standard Treatment — systematic review and meta-analysis. Current Neuropharmacology. https://pubmed.ncbi.nlm.nih.gov/37519000/
- Filippini, G., Minozzi, S., Borrelli, F., et al. (2022). Cannabis and cannabinoids for symptomatic treatment for people with multiple sclerosis — Cochrane systematic review. Cochrane Database of Systematic Reviews. https://pubmed.ncbi.nlm.nih.gov/35510826/
- (2026). Cannabis-based medicines for chronic neuropathic pain in adults — Cochrane systematic review. Cochrane Database of Systematic Reviews. https://pubmed.ncbi.nlm.nih.gov/41548880/
- Smith, L. A., Azariah, F., Lavender, V. T., et al. (2015). Cannabinoids for nausea and vomiting in adults with cancer receiving chemotherapy — Cochrane systematic review. Cochrane Database of Systematic Reviews. https://pubmed.ncbi.nlm.nih.gov/26561338/
- Bergamaschi, M. M., Queiroz, R. H., Chagas, M. H., et al. (2011). Cannabidiol reduces the anxiety induced by simulated public speaking in treatment-naive social phobia patients — randomised controlled trial. Neuropsychopharmacology. https://pubmed.ncbi.nlm.nih.gov/21307846/
- Freeman, T. P., Hindocha, C., Baio, G., et al. (2020). Cannabidiol for the treatment of cannabis use disorder: a phase 2a, double-blind, placebo-controlled, randomised trial. The Lancet Psychiatry. https://pubmed.ncbi.nlm.nih.gov/32735782/
- Naftali, T., Bar-Lev Schleider, L., Almog, S., et al. (2021). Oral CBD-rich Cannabis Induces Clinical but Not Endoscopic Response in Patients with Crohn’s Disease — randomised controlled trial. Journal of Crohn’s & Colitis. https://pubmed.ncbi.nlm.nih.gov/33858011/
- (2025). Cannabis use in Crohn’s disease: a systematic review and meta-analysis of randomised controlled trials. Irish Journal of Medical Science. https://pubmed.ncbi.nlm.nih.gov/39821383/
- Mücke, M., Weier, M., Carter, C., et al. (2018). Systematic review and meta-analysis of cannabinoids in palliative medicine. Journal of Cachexia, Sarcopenia and Muscle. https://pubmed.ncbi.nlm.nih.gov/29400010/
- (2022). Efficacy of medicinal cannabis for appetite-related symptoms in people with cancer — systematic review and meta-analysis. Palliative Medicine. https://pubmed.ncbi.nlm.nih.gov/35360989/
- (2024). Effects of a cannabidiol/terpene formulation on sleep in individuals with insomnia: a double-blind, placebo-controlled randomised trial. Journal of Clinical Sleep Medicine. https://pubmed.ncbi.nlm.nih.gov/39167421/
- (2025). Effectiveness of cannabinoids on subjective sleep quality in people with and without insomnia — systematic review and meta-analysis. Sleep Medicine Reviews. https://pubmed.ncbi.nlm.nih.gov/40929927/
- Müller-Vahl, K. R., Pisarenko, A., Fremer, C., et al. (2023). CANNA-TICS: Efficacy and safety of oral treatment with nabiximols in adults with chronic tic disorders — randomised controlled trial. Psychiatry Research. https://pubmed.ncbi.nlm.nih.gov/36878177/
- (2026). Single oral administration of dronabinol increases ocular blood flow in patients with glaucoma — randomised controlled trial. Acta Ophthalmologica. https://pubmed.ncbi.nlm.nih.gov/40772417/
- Guzmán, M., Duarte, M. J., Blázquez, C., et al. (2006). A pilot clinical study of delta-9-tetrahydrocannabinol in patients with recurrent glioblastoma multiforme — clinical trial. British Journal of Cancer. https://pubmed.ncbi.nlm.nih.gov/16804518/
- (2025). Mechanisms of Cell Death Induced by Cannabidiol Against Tumor Cells: A Review of Preclinical Studies. Plants. https://pubmed.ncbi.nlm.nih.gov/40006844/
- (2023). Cannabis-based medicines and medical cannabis for adults with cancer pain — Cochrane systematic review. Cochrane Database of Systematic Reviews. https://pubmed.ncbi.nlm.nih.gov/37283486/
- Marconi, A., Di Forti, M., Lewis, C. M., et al. (2016). Meta-analysis of the Association Between the Level of Cannabis Use and Risk of Psychosis. Schizophrenia Bulletin. https://pubmed.ncbi.nlm.nih.gov/26884547/
- (2025). Fetal Cannabis Exposure and Neonatal Outcomes: A Systematic Review and Meta-Analysis. Maternal and Child Health Journal. https://pubmed.ncbi.nlm.nih.gov/40317448/
- Braun, I. M., Bohlke, K., Abrams, D. I., et al. (2024). Cannabis and Cannabinoids in Adults With Cancer: ASCO Guideline — practice guideline. Journal of Clinical Oncology. https://pubmed.ncbi.nlm.nih.gov/38478773/