Conditions
Alzheimer's Disease: An Overview
An overview of Alzheimer's disease — its stages, what actually goes wrong in the brain (amyloid, tau, and the acetylcholine story sorted out), how the newer anti-amyloid drugs work, and an honest look at the herbs and supplements studied for cognitive support.
December 30, 2016 · updated July 3, 2026

Alzheimer’s disease is a neurodegenerative disorder that lowers the brain’s ability to access and store memories.
It’s a condition that exponentially worsens over time and will eventually result in death.
The purpose of this article is to serve as an overview of the condition for anybody looking for more information.
There Are 3 stages of Alzheimer’s:
1. The First Stage:
Alzheimer’s begins with mild disorientation and difficulty with memories.
These memories are usually only new memories, such as where the car keys are, what happened the day before, and the names of people met recently.
This is associated with damage in the hippocampus region in the brain which serves long-term memory.
Other symptoms of the first stage include:
- Difficulty finding the right words
- Trouble remembering recently read material
- Inability to put names to faces of people
- Trouble with planning
- Overall reduction in short term memory
2. The Second Stage
As the condition progresses, the damage can be found further throughout the brain, up to the cerebral cortex.
When this begins to take place, the symptoms will begin to grow stronger.
Memories from the past will become lost as the neurons are destroyed. This stage affects more than just the formation of new memories, it will affect memories from as far back as childhood.
Symptoms in the second stage includes:
- Forgetting events from personal history
- Moodiness or antisocial behaviour towards challenging situations
- Confusion about the time and place they are in
- Sleep pattern issues, insomnia and tiredness at different points in the day
- Becoming lost easily
- Personality or behavioural changes
3. The Third Stage
The last stage occurs after a significant neuronal loss in the brain.
The brain will have visible shrinkage from a great deal of lost neurons.
All normal function will become lost, and the person will need assistance with normal daily activities like getting out of bed, bathing and going to the bathroom.
Communication will be difficult, and the person will have a very hard time avoiding confusion and frustration.
In symptoms of the third (and final stage) of Alzheimer’s:
- They require around the clock care and assistance with nearly all daily activities
- They will experience difficulty sitting, standing, and lying normally
- Communication will be limited and difficult
- They will be vulnerable to infections
- They will lose the ability to recognize faces, including close friends and family
- They will become confused and frustrated on a daily basis
What Causes Alzheimer’s Disease?
Alzheimer’s can have a long list of causes, and scientists have long been in disagreement over the actual cause of the condition.
Some frame it as a metabolic disorder — the so-called “type 3 diabetes” idea, where brain cells become resistant to insulin — while others emphasise inherited genetic risk. Most researchers now see it as a mix of both, plus age and lifestyle.
Recently there have been some good quality studies with new information regarding the cause of Alzheimer’s.
In the brain, Alzheimer’s has been found to show the first signs of damage in the hippocampus.
This is the region of the brain that plays a key role in memory storage, as well as imagining events in the future. It is closely related to constructing visual locations of past and future places and events.
It also happens to be the first place damage is noticed in the progression of Alzheimer’s. If enough damage occurs in the hippocampus, disorientation and difficulty storing new memories will result. Both of which are early markers for Alzheimer’s disease.
Over time, this damage can be seen spreading throughout the brain. On the microscopic level, this shows up as tangles in a protein called tau — normally tau stabilises the tiny internal “tracks” that move cargo around a neuron, but in Alzheimer’s it clumps into tangles that choke the cell’s ability to function.
The other hallmark is the buildup of a sticky fragment called amyloid-beta. This is produced when a larger protein sitting in the neuron’s membrane, called amyloid precursor protein (APP), is cut up by enzymes known as secretases 1Reference 1The amyloid hypothesis of Alzheimer’s disease at 25 years. Normally the fragments are cleared away; in Alzheimer’s they clump together into plaques between the neurons instead. Over time, both the tau tangles inside cells and the amyloid plaques outside them are associated with the death of neurons.
When this happens on a large scale, throughout the brain, as in the case of Alzheimer’s, this can actually be seen with the naked eye as the brain shrinks in size. As the neurons die, large amounts of brain tissue are lost and the brain begins to shrink, mainly from the cerebral cortex where the bulk of the gray matter is located.
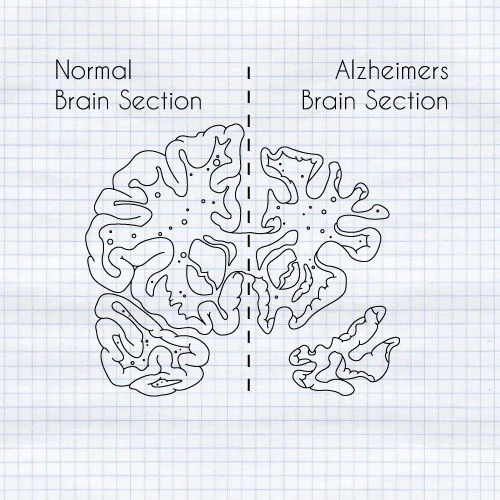
The size difference is due to a massive loss of neurons, mainly from the cerebrum.
Can Alzheimer’s Be Detected Early On?
In recent years, as the field of neuroscience forms a deeper level of understanding about complexities of the human brain, new theories are being tested on how we can identify Alzheimer’s before it becomes irreversible.
In one study, researchers from the University of Aberdeen identified key changes in the brains of people with Alzheimer’s disease.
They confirmed that the two proteins (amyloid and tau) both play a significant role in the disease, and reported an interaction between the two 2Reference 2Early Signs of Alzheimer’s Identified.
With this information, researchers are able to develop new techniques that we can use to test for an abnormal presence of these proteins to look for Alzheimer’s before it becomes irreversible.
Another marker being studied is the enzyme monoamine oxidase B (MAO-B). MAO-B breaks down monoamine neurotransmitters like dopamine and, as a by-product of that reaction, generates hydrogen peroxide and other reactive molecules that can stress neurons.
In Alzheimer’s, MAO-B is markedly elevated in reactive astrocytes — support cells that swell up and cluster around amyloid plaques — and the amount tends to track with the local damage 3Reference 3ReviewNam, M. H., et al. A Key Mediator and Imaging Target in Alzheimer’s Disease: Unlocking the Role of Reactive Astrogliosis Through MAO-B. (Review.) PMC. Link. That has made MAO-B an active target for PET brain imaging, as a way to detect the reactive changes around plaques earlier in the disease process.
What to take away from this
As these studies are analysed further, markers such as tau, amyloid-beta, and MAO-B are all being explored as signals of the early stages of Alzheimer’s.
From here, we can develop ways to measure this without having to dissect the brain under a microscope.
If we can develop blood tests, cerebrospinal fluid tests, or MRI techniques to identify the presence of these proteins in elevated levels, then we may be able to detect Alzheimer’s long before it becomes a problem.
The next big leap will be to develop diagnostic techniques with this information, to check for these markers early on in the disease process, and promptly treating it.
Areas To Focus On for Prevention And Treatment
Using this information, we know that Alzheimer’s is associated with a buildup of amyloid and MAO-B, along with the tangling of tau proteins.
Finding ways to prevent or reverse these processes will be important in the treatment of Alzheimer’s disease in the long term.
Although not widely tested yet in the scientific literature, it is likely that the best way treat or prevent Alzheimer’s is through daily supplementation and lifestyle changes. As with most chronic illnesses, this condition is not a simple issue. It’s a long-term, gradual destruction of the neurons in the brain. Therefore, when talking about prevention, a long-term, regular strategy will be necessary.
Neurotransmitter modulators, adequate blood flow, water intake, nutritional support, and stress reduction techniques all have a beneficial impact on both the treatment and prevention of Alzheimer’s.
Let’s discuss some of these main mechanisms in more detail…
1. Amyloid Plaquing
Amyloid-beta is produced when a larger protein called amyloid precursor protein (APP) is cut into fragments inside the neuron. As we age, more of this byproduct tends to accumulate, and in Alzheimer’s the fragments clump together into plaques instead of being cleared away.
It’s worth being clear about a common point of confusion here: amyloid-beta does not come from the breakdown of acetylcholine. It comes from APP. Many traditional memory remedies act on acetylcholine instead, by slowing the enzyme acetylcholinesterase (which breaks acetylcholine down). Inhibiting that enzyme raises acetylcholine levels — which can ease symptoms by supporting memory and communication between neurons — but it does not slow the underlying disease or reduce how much amyloid the brain produces 4Reference 4Systematic reviewCholinesterase inhibitors for Alzheimer’s disease.
Why mention these herbs in the same breath as amyloid, then? Because acetylcholinesterase inhibition is the mechanism most of the older Alzheimer’s drugs share (donepezil, galantamine, rivastigmine), and several plants act on the same enzyme. Adequate cerebral blood flow and antioxidant support are the angles more often tied to amyloid itself. A newer class of drugs takes aim at the plaques more directly: anti-amyloid antibodies. The first, aducanumab (Aduhelm), was approved in 2021 amid heavy controversy and then withdrawn from the market in 2024 5Reference 5Aducanumab to be Discontinued as an Alzheimer’s Treatment. Two successors — lecanemab (Leqembi, 2023) and donanemab (Kisunla, 2024) — are now FDA-approved and do modestly slow decline in early Alzheimer’s, though they carry real risks (brain swelling and small bleeds) and are not cures 6Reference 6FDA approves third anti-amyloid antibody for Alzheimer disease.
Compounds studied for acetylcholine support:
- Huperzine-A (from Huperzia serrata)
- Muira puama (Ptychopetalum olacoides)
- Bacopa (Bacopa monnieri)
- Coleus (Coleus forskohlii)
- Galantamine (originally from Galanthus, the snowdrop)
2. MAO (Monoamine oxidase)
Monoamine oxidase breaks down the monoamine neurotransmitters — dopamine, norepinephrine, and serotonin.
There’s genuine interest in MAO-B inhibition as an angle in neurodegeneration: MAO-B climbs in the ageing brain, and blocking it lowers the reactive by-products described earlier. The prescription MAO-B inhibitor selegiline has been trialled in Alzheimer’s, but the evidence for a lasting benefit has been underwhelming — so this is best read as a research direction, not an established treatment.
Several plants contain natural MAO inhibitors, though most have been studied for mood rather than dementia:
- Passionflower (Passiflora spp.)
- Ayahuasca vine (Banisteriopsis caapi) — its harmala alkaloids are reversible MAO-A inhibitors
- Ginkgo (Ginkgo biloba)
- Rhodiola (Rhodiola rosea)
3. Stress
When looking at the process that takes place in the progression of Alzheimer’s, it’s well known that stress plays a major factor.
In the hippocampus, where the progression of Alzheimer’s begins, there is a high level of glucocorticoid receptors present.
These are special receptors that pick up and respond to the stress hormones within the body such as cortisol.
In the short term, the effects brought on by this is beneficial and well designed to improve survival in stressful situations.
In the long term, however, as with chronic stress conditions, this can have major negative consequences on the body, and though we are not sure if this is enough to cause Alzheimer’s, it will do nothing to prevent it. In fact, it is likely to exponentiate the effects of Alzheimer’s progression in the hippocampus through mutual damage.
The best ways to reduce stress includes:
- Adequate exercise (20 min-1 hour a day)
- Regular water consumption
- Meditation
- Adequate sleep
- Avoiding added sugar
- Seeing family and friends regularly (socializing)
- Taking time to be alone and away from the computer
Herbs and supplements studied for cognitive support
A number of herbs and supplements have been studied for cognitive support, often because they act on one of the mechanisms above — slowing the breakdown of acetylcholine, supplying its building blocks, supporting blood flow, or fighting oxidative damage.
An important caveat: the evidence here is preliminary. Most of these have small or early-stage studies behind them, not the kind of large, long-term trials needed to say anything is proven to prevent or treat Alzheimer’s. None of this is a substitute for medical care. Think of the list below as “what’s been looked at,” not “what works.”
-
Huperzine-A (Huperzia serrata, Chinese club moss) — a compound traditionally used in Chinese medicine that slows acetylcholinesterase, the enzyme that breaks down acetylcholine. It’s potent by weight (active in the microgram range) and has been studied as a milder-side-effect alternative to some prescription cholinesterase inhibitors. The evidence is preliminary — a Cochrane review found the existing trials too small and low in quality to draw firm conclusions 7Reference 7Systematic reviewHuperzine A for Alzheimer’s disease — insufficient evidence.
-
Alpha-GPC — a choline compound that crosses the blood-brain barrier and supplies choline, a raw material the brain uses to make acetylcholine. It’s often paired with acetylcholinesterase-acting compounds on the theory that supply plus slower breakdown work better together. A multicentre double-blind trial in mild-to-moderate Alzheimer’s reported cognitive benefits 8Reference 8RCTCognitive improvement in mild to moderate Alzheimer’s dementia after treatment with the acetylcholine precursor choline alfoscerate (alpha-GPC): a multicenter, double-blind, randomized, placebo-controlled trial, but this remains an early and limited body of evidence.
-
Muira puama (Ptychopetalum olacoides) — an Amazonian herb traditionally used for memory and age-related complaints. It has been reported to inhibit acetylcholinesterase. Traditionally it was paired with catuaba for “age-related disorders.” Evidence is largely traditional and preliminary.
-
Catuaba (Trichilia catigua) — traditionally combined with muira puama. Early studies suggest it acts on the brain’s dopamine system, which may relate to mood and behavioural symptoms in dementia. Preliminary.
-
Periwinkle / vinpocetine (Vinca minor) — periwinkle contains vincamine, the basis for the semi-synthetic compound vinpocetine. It crosses the blood-brain barrier and has been studied for effects on cerebral blood flow and brain metabolism. Proposed actions include improving blood flow and protecting neurons; the supporting evidence is preliminary.
-
Ginkgo (Ginkgo biloba) — long used in traditional Chinese medicine for age-related memory loss, and one of the more researched herbs for cognitive ageing. It’s been studied for antioxidant, anti-inflammatory, and blood-flow effects — but the two largest prevention trials (the GEM study and GuidAge) found it did not reduce the risk of developing dementia 9Reference 9RCTGinkgo biloba for prevention of dementia (Ginkgo Evaluation of Memory / GEM Study): a randomized controlled trial10Reference 10RCTLong-term use of standardised Ginkgo biloba extract for the prevention of Alzheimer’s disease (GuidAge): a randomised placebo-controlled trial. Any benefit, if there is one, is modest.
-
Sage (Salvia officinalis) — traditionally used “to improve the mind.” Some studies report it inhibits acetylcholinesterase, similar in direction to several herbs above. Preliminary.
-
Cat’s claw (Uncaria tomentosa) — researchers have reported that an alkaloid from cat’s claw (mitraphylline) can bind beta-amyloid in the lab, which has been proposed as a way to make the protein easier to clear. This is early, mostly preclinical work.
-
Turmeric / curcumin (Curcuma longa) — the curcuminoids in turmeric have been studied as antioxidants and for possible effects on beta-amyloid. Interest is high but human evidence for cognitive benefit remains preliminary, and curcumin is famously poorly absorbed.
-
Bacopa (Bacopa monnieri) — a traditional Ayurvedic herb studied for memory and learning, with proposed antioxidant and acetylcholine-related actions. Preliminary.
A few others sometimes included in this conversation for their antioxidant or nutritional roles: DHA (an omega-3 fat), coenzyme Q10, L-theanine, and the B vitamins (B6, B12). As with everything above, these are areas of study and general nutritional support — not established Alzheimer’s treatments.
Author
The Sunlight Experiment
References
- Selkoe, D. J., & Hardy, J. (2016). The amyloid hypothesis of Alzheimer’s disease at 25 years. EMBO Molecular Medicine, 8(6), 595–608. Link
- University of Aberdeen. (2016). Early Signs of Alzheimer’s Identified. Neuroscience News. Link
- Nam, M. H., et al. A Key Mediator and Imaging Target in Alzheimer’s Disease: Unlocking the Role of Reactive Astrogliosis Through MAO-B. (Review.) PMC. Link
- Birks, J. (2006). Cholinesterase inhibitors for Alzheimer’s disease. Cochrane Database of Systematic Reviews, (1), CD005593. Link
- Alzheimer’s Association. Aducanumab to be Discontinued as an Alzheimer’s Treatment. Link
- Mullard, A. (2024). FDA approves third anti-amyloid antibody for Alzheimer disease. Nature Reviews Drug Discovery. Link
- Yang, G., et al. (2013). Huperzine A for Alzheimer’s disease — insufficient evidence. Cochrane Database of Systematic Reviews, CD005592. Link
- De Jesus Moreno Moreno, M. (2003). Cognitive improvement in mild to moderate Alzheimer’s dementia after treatment with the acetylcholine precursor choline alfoscerate (alpha-GPC): a multicenter, double-blind, randomized, placebo-controlled trial. Clinical Therapeutics, 25(1), 178–193. Link
- DeKosky, S. T., et al. (2008). Ginkgo biloba for prevention of dementia (Ginkgo Evaluation of Memory / GEM Study): a randomized controlled trial. JAMA, 300(19), 2253–2262. Link
- Vellas, B., et al. (2012). Long-term use of standardised Ginkgo biloba extract for the prevention of Alzheimer’s disease (GuidAge): a randomised placebo-controlled trial. The Lancet Neurology, 11(10), 851–859. Link